
Estimated Read Time: 10–15 minutes
Summary: Mast Cell Activation Syndrome (MCAS) is a complex, multisystem condition requiring layered care. This article reviews medications commonly prescribed for mast cell activation syndrome, including stabilizers, antihistamines, leukotriene blockers, and adjunct therapies. It highlights the importance of tolerability and explains how compounded formulations allow prescribers to customize strengths, dosage forms, and excipients to better support oftentimes sensitive MCAS patients.
- Why Commercially Available Medications Aren’t Always Enough
- Understanding Mast Cell Activation Syndrome (MCAS)
- How Practitioners Manage Patients’ MCAS
- Medication Strategies in Mast Cell Activation Syndrome (MCAS)
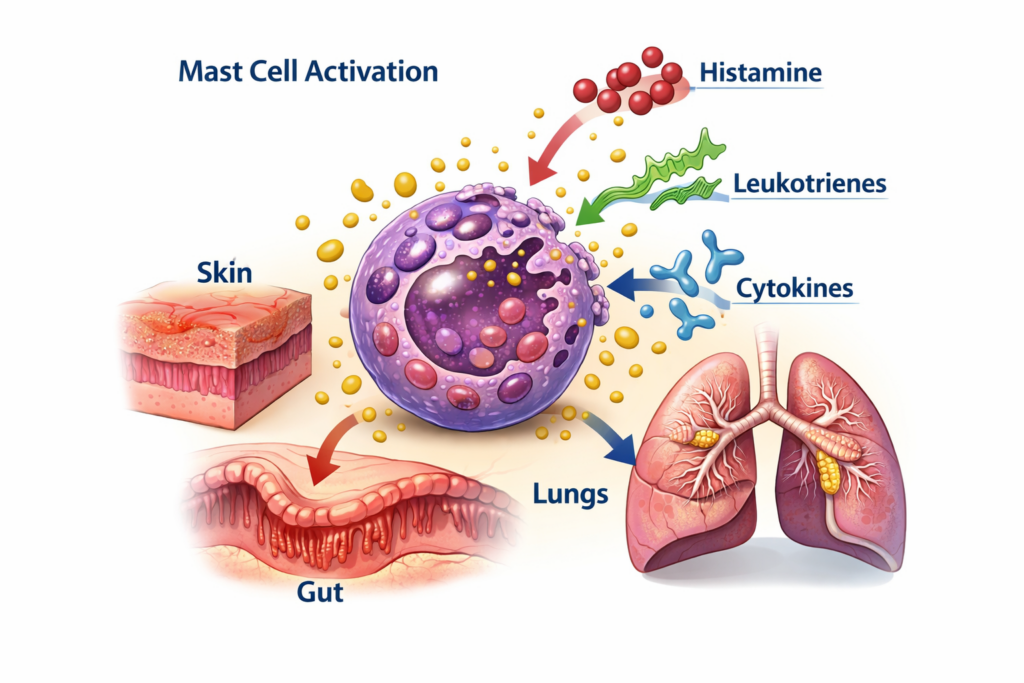
Mast Cell Activation Syndrome (MCAS) is a complex and often misunderstood condition in which mast cells release excessive or inappropriate amounts of inflammatory mediators.
These mediators — including histamine, prostaglandins, leukotrienes, cytokines, and tryptase — can affect nearly every organ system in the body.
Patients with MCAS may experience:
- Flushing
- Urticaria (hives) and itching
- Gastrointestinal distress
- Brain fog
- Tachycardia
- Headaches
- Hypotension
- Respiratory symptoms
- Anaphylactoid reactions

Because mast cells reside throughout connective tissues, symptoms are often multisystem, variable, and unpredictable. For both patients and providers, management can be challenging.
In clinical practice, many of the medications used in Mast Cell Activation Syndrome are either not commercially available in appropriate oral strengths or require modification due to excipient sensitivity. As a result, compounding pharmacies may play a central role in implementing safe and sustainable MCAS therapy plans.
Why Commercially Available Medications Aren’t Always Enough
Managing Mast Cell Activation Syndrome (MCAS) requires more than simply selecting the “right” medication class. For many patients, the challenge is not just what drug is prescribed — but how it is formulated, dosed, and tolerated.
Individuals with MCAS are often highly sensitive not only to environmental triggers, but also to inactive ingredients commonly found in commercially manufactured medications. Dyes, preservatives, fillers, binders, and excipients may provoke symptoms rather than relieve them. A medication that is pharmacologically appropriate may still fail clinically if it increases reactivity.
In addition, commercially available products may present other limitations:
- Fixed dosing that does not allow for gradual titration
- Lack of preservative-free or dye-free options
- Absence of certain medications in oral form in the United States
- Limited flexibility in combining therapies to match multisystem symptom patterns

In many MCAS cases, therapies cannot be fully implemented using commercially manufactured products alone. Certain medications — such as oral ketotifen — are not available in the United States and must be compounded for systemic use. Others may technically be available but require removal of dyes, preservatives, or fillers that trigger reactivity. Compounding allows prescribers to execute therapeutic strategies that would otherwise be limited by formulation constraints.
Compounded preparations allow clinicians to tailor therapy — adjusting strength, removing reactive excipients, and selecting dosage forms that align with the patient’s tolerance and clinical presentation.
Commonly Compounded Mast Cell Stabilizers, Antihistamines & Adjunct Therapies in MCAS
Below is an overview of commonly used medications in Mast Cell Activation Syndrome (MCAS) management:
- Cromolyn Sodium
- Ketotifen
- Hydroxyzine
- Diphenhydramine
- Cyproheptadine
- Montelukast
- Famotidine
- Low Dose Naltrexone (LDN)
- Quercetin (pharmaceutical-grade)
- Luteolin
- Montelukast
Let’s explore how each of these medications works, when they are prescribed, and how compounded formulations may support patients in MCAS care.
Understanding Mast Cell Activation Syndrome (MCAS)
First, let’s understand what is happening in MCAS. Mast cells are specialized immune cells that act as your body’s first responders. Their job is to release chemicals like histamine and leukotrienes upon detecting a pathogen, allergen, or injury. This is a normal part of your immune defense.
But when they become hyper-responsive, mast cells may release these chemicals too easily, too intensely, or at random.
Because they reside in connective tissues, this unusual activity can cause chaos across organ systems and lead to:
- Skin: Hives, itching, flushing, or swelling.
- Digestion: Cramping, diarrhea, reflux, or food intolerance.
- Respiratory: Congestion, throat tightness, or wheezing sensations.
- Neurological: Headaches, nerve pain, or insomnia.
- Systemic: Fatigue, dizziness, or flares triggered by stress, heat, or specific foods.
However, having a single symptom or even frequent hives doesn’t automatically lead to MCAS. The pattern is what raises suspicion for physicians. They look for symptoms that cluster and flare with broad triggers but improve when mast cells are stabilized.
How Practitioners Manage Patients’ MCAS
When clinicians suspect mast cell involvement, careful evaluation and a structured management strategy are essential. Because MCAS is multifactorial and highly individualized, care plans are typically layered and strategic rather than single-drug solutions.
This layered approach helps patients know what to take daily, what to use during a flare, and when symptoms require stronger intervention.
A sustainable plan distinguishes between:
- Baseline Therapy:
Daily medications used to maintain mast cell stability, reduce mediator release, and minimize flare frequency. These typically include mast cell stabilizers and histamine pathway blockers taken consistently. - Targeted Pathway Support:
Add-on therapies layered onto baseline therapy when symptoms suggest involvement of specific mediator pathways (e.g., leukotrienes or serotonin). - Rescue Therapy:
Fast-acting medications used as needed to interrupt acute histamine-mediated flares, such as sudden hives, itching, flushing, or mild allergic-type reactions. - Escalation Therapy:
Higher-intensity interventions reserved for refractory or severe symptom flares and used under close clinical supervision. - Adjunct/Burden Support:
Supportive therapies that do not directly stabilize mast cells but may reduce overall inflammatory, neurologic, or pain-related burden in complex cases.
In MCAS management, tolerability can be as important as mechanism. A medication that works “on paper” may fail in practice if excipients provoke symptoms or if standard dosing exceeds a patient’s activation threshold.
Fortunately, patients have options in compounding that allow their providers to develop customized plans to match their sensitivities.
Compounded Medication Strategies in Mast Cell Activation Syndrome (MCAS)
A sustainable Mast Cell Activation Syndrome (MCAS) plan is not built around isolated prescriptions. It is built around clearly defined medication roles, thoughtful sequencing, and formulation strategies that respect patient sensitivity.
Below is a more detailed look at how each medication layer functions — and how compounding pharmacy may support clinical precision at every step.
Baseline Therapy
Daily medications used to maintain mast cell stability and reduce flare frequency.
Most patients begin with a foundational regimen designed to stabilize mast cells and block mediator effects. The goal is to minimize inappropriate mediator release and reduce baseline reactivity.
Cromolyn Sodium
Mast Cell Stabilizer
Foundational, mast-cell-targeting option often used when symptoms suggest broad mediator release, especially with GI involvement.
- Commonly considered for abdominal pain, diarrhea, nausea, flushing, and “reactive” multisystem patterns.
- Often introduced with slow titration, and compounded options may improve tolerability for excipient-sensitive patients.
- Multiple studies support cromolyn’s role in stabilizing mast cells in systemic and GI-predominant mast cell disorders.
Ketotifen
H1 + Mast Cell Stabilizer
Ketotifen is frequently used as a foundational mast cell stabilizer in patients with multisystem symptoms.
As both an H1 antihistamine and mast cell stabilizing agent, it may support symptom control across multiple organ systems, including:
- Gastrointestinal tract
- Skin
- Respiratory system

Because mast cells are widely distributed throughout connective tissues, ketotifen is often incorporated when broader systemic stability is needed.
An 8-week randomized controlled study in patients with irritable bowel syndrome demonstrated that ketotifen reduced visceral hypersensitivity and improved abdominal symptoms, supporting its role in mast cell–mediated gastrointestinal conditions.
Ketotifen is not commercially manufactured as an oral prescription product in the United States. For systemic use, it must be compounded.
This makes compounding pharmacy potentially helpful in implementing ketotifen-based MCAS protocols. It allows prescribers to:
- Customize dosing strength
- Initiate gradual titration
- Remove reactive excipients
- Select capsule, liquid, or alternative delivery forms
Famotidine
H2 Receptor Blocker
- Used alongside H1 blockade to reduce histamine-mediated GI and vascular symptoms.
- Often selected for reflux, abdominal discomfort, flushing, and broader histamine patterns.
- Common part of foundational daily therapy.
- Clinical trials evaluating famotidine in acute urticaria have demonstrated symptom reduction when used alone or alongside H1 blockers, supporting its complementary role in histamine pathway control.
When commercial formulations contain reactive fillers or dyes, compounded options may improve tolerability.
Hydroxyzine
Sedating H1 Blocker
- Option when histamine-type symptoms persist, especially when sedation at night is clinically useful.
- Commonly considered for itching, hives, flushing, and sleep disruption related to histamine activity.
- Often individualized due to sedation, and compounded options may help avoid dyes/fillers in sensitive patients.
- A randomized, double-blind study compared cetirizine vs hydroxyzine vs placebo in chronic idiopathic urticaria.
Because baseline stabilization must be taken consistently and long term, tolerability is critical. Compounded preparations often allow prescribers to initiate therapy at lower strengths than commercially available options and gradually titrate upward — a strategy that may reduce activation risk in highly reactive patients.
Rescue Therapy
Fast-acting agents used as needed to interrupt acute flares.
Diphenhydramine
Rapid-Acting H1 Blocker
- Used as-needed for acute histamine-type flares rather than daily stability.
- Common rescue option for sudden/acute hives, itching, flushing, and mild histamine-mediated reactions.
- Short duration of action and sedating profile limit use as maintenance therapy.
- May serve as adjunctive support in allergic reactions but does not replace epinephrine in anaphylaxis.
- Randomized clinical studies in acute urticaria have shown diphenhydramine effectively reduces itch and wheal formation, supporting its role as short-term rescue therapy.
Targeted Pathway Support
Add-on therapies addressing specific mediator pathways when baseline therapy is insufficient.
If certain symptoms dominate, clinicians may target specific inflammatory mediator pathways rather than broadly intensifying all therapy.
For example, montelukast may be added to block leukotriene receptors in patients with prominent respiratory symptoms such as wheezing, chest tightness, or exercise intolerance.
Montelukast
Leukotriene Receptor Antagonist
Montelukast is often used as add-on mediator pathway support in patients whose symptoms are not fully controlled with H1 and H2 blockade alone. It works by blocking the cysteinyl leukotriene (CysLT1) receptor, helping reduce leukotriene-driven inflammation.
Clinically, it may be particularly helpful in patients with:
- Wheezing or respiratory symptoms
- Persistent hives or itching
- Abdominal cramping related to smooth muscle activation
Studies in chronic idiopathic urticaria have shown that montelukast may reduce itch severity and hive frequency in some patients, particularly when used as adjunctive therapy.
Cyproheptadine
H1 Blocker with Serotonin Antagonism
- Considered in select cases where histamine and serotonin pathways may both contribute to symptoms.
- May be used for itching, flushing, headaches, and certain GI symptom patterns.
- A randomized placebo-controlled trial in pediatric functional abdominal pain demonstrated symptom improvement with cyproheptadine, supporting its role in select GI-related hypersensitivity patterns.
Escalation Therapy
Higher-intensity interventions reserved for refractory or severe flares.
Budesonide
GI-Directed Corticosteroid
- Considered when symptoms suggest intestinal inflammation alongside mast cell involvement.
- May be used in persistent diarrhea or inflammatory-leaning GI flares not responsive to foundational therapy.
- Typically employed as part of a clinician-directed escalation plan.
- In a report of refractory mastocytic enterocolitis, oral budesonide demonstrated potential in managing abdominal pain and diarrhea.

Adjunct/Symptom Burden Support
Therapies that do not directly target mast cells but may reduce overall inflammatory or neurologic burden.
Compounded Low-Dose Naltrexone
Off-Label Immune/Neuroimmune Modulator
- Low-Dose Naltrexone (LDN) is sometimes incorporated as a select-case adjunct when the clinical picture is complex or symptoms persist despite standard mast cell–directed therapy. Its use is off-label and should be guided by careful clinical judgment.
- LDN is most often considered in patients with refractory, multisystem presentations where broader neuroimmune or immunomodulatory strategies are being explored.
- While large-scale randomized trials in MCAS are limited, case-report literature describes improvement in patients with overlapping conditions such as MCAS and severe postural orthostatic tachycardia syndrome (POTS) when naltrexone was included as part of a comprehensive care plan. These reports suggest potential benefit in select individuals, though more research is needed.




Compounded low-dose naltrexone is necessary to achieve the micro-dose strengths not available in standard commercial products.
Many adjunct strategies used in complex MCAS care — including low-dose naltrexone — require strengths that are not commercially manufactured. In these cases, compounding pharmacy is not simply a convenience but a structural necessity for appropriate dosing.
Gabapentin
Neuromodulator + Mast Cell Stabilizer
Gabapentin’s role in Mast Cell Activation Syndrome (MCAS) care is increasingly understood through two complementary mechanisms:
- Modulation of central and peripheral sensitization
- Potential mast cell–modulating effects within the gastrointestinal tract
Because of the current rise in utilization, let’s go deeper into the mechanism of action of Gabapentin.
1. Central Sensitization & Neuropathic Signaling
Gabapentin reduces excitatory neurotransmitter release (including glutamate), it decreases neuronal hyperexcitability.
In patients with MCAS, ongoing mediator release (histamine, prostaglandins, leukotrienes, cytokines) can drive:
- Visceral hypersensitivity
- Chronic neuropathic-type pain
- Heightened itch signaling
- Sleep disruption
- Central amplification of sensory input
Even when mast cell activity is partially controlled, neural sensitization may persist. Gabapentin helps dampen this amplified pain and itch signaling at the spinal and supraspinal levels.
This explains why gabapentin is sometimes used in MCAS patients with:
- Neuropathic pain
- Burning or tingling sensations
- Refractory pruritus (uncomfortable skin sensation that causes an urge to scratch)
- “Pain out of proportion” to objective findings
- Sleep disturbance driven by discomfort
Randomized controlled trials in other populations (including uremic pruritus and neuropathic itch) demonstrate significant reductions in itch severity, supporting its role in centrally mediated pruritus.
2. Evidence: Gabapentin and Mast Cells in the Colon
Beyond neuromodulation, experimental research suggests gabapentin may influence mast-cell-associated inflammation within the gastrointestinal tract.
A 2020 preclinical study evaluating gabapentin in an experimental colitis model demonstrated:
- Reduced visceral hypersensitivity
- Decreased inflammatory signaling
- Reduced mast cell density and activation markers in colonic tissue
- Downregulation of pro-inflammatory pathways (including NF-κB signaling)
Mast cells and enteric nerves communicate bidirectionally in the gut. Activated mast cells release histamine, tryptase, prostaglandins, and cytokines that sensitize nearby nociceptive fibers. In turn, activated nerves can stimulate further mast cell degranulation — creating a feed-forward cycle of pain and reactivity.
Gabapentin appears to interrupt this neuro-immune loop.
In colonic tissue models, gabapentin was associated with:
- Reduced mast cell density or activation markers
- Decreased release of inflammatory mediators
- Improvement in visceral pain signaling
These findings suggest gabapentin may exert indirect mast cell–regulating effects within colonic tissue in experimental models. When lower starting doses or dye-free formulations are required, compounded preparations may improve tolerability in sensitive patients.
Why This Matters in MCAS
Many MCAS patients present with:
- Abdominal pain with hypersensitivity quality
- Post-prandial flares
- IBS-like patterns
- Burning GI discomfort without structural pathology
- Persistent symptoms despite antihistamines and mast cell stabilizers
In these scenarios, symptoms may reflect mast cell–nerve cross-talk rather than uncontrolled mediator release alone.
Gabapentin may help by:
- Reducing neural amplification of mast cell signaling
- Dampening mast cell–nerve signaling loops
- Improving visceral pain thresholds
- Supporting sleep restoration (which can reduce flare frequency)
This positions gabapentin as adjunct burden-reduction therapy.
Quercetin (Pharmaceutical-Grade)
Flavonoid which modulates Mast Cells
- Adjunct supportive option often used for its mast-cell–modulating and antioxidant properties.
- Commonly considered for seasonal flare patterns, histamine sensitivity, and skin/upper-airway symptom profiles.
- Consistency of sourcing and dosing matters; “pharmaceutical-grade” helps reduce variability.
- Randomized controlled trials in allergic populations have shown quercetin supplementation reduced symptom scores, supporting its potential mast cell–modulating and antihistamine effects.
Luteolin
Flavonoid/Neuroinflammatory Support
- Adjunct supportive flavonoid often discussed for mast-cell–modulating and anti-inflammatory properties (evidence base is still emerging).
- Sometimes considered when brain fog/headache or inflammatory sensitivity are prominent alongside mast-cell symptoms.
- Best positioned as supportive rather than foundational therapy, with careful product selection and monitoring.
- Preclinical and mechanistic studies demonstrate that luteolin inhibits mast cell activation and mediator release, providing biologic rationale for its adjunctive use in mast cell–related conditions.
Hypothetical MCAS Scenarios Using Compounded Strategies
Clinical Situations Where MCAS May Be in Play
Immunologist
- Episodic urticaria and pruritus, flushing-type episodes, and flare days that escalate fast.
- The regimen is built in lanes. Ketotifen is the stabilization foundation. Montelukast is layered in when the urticaria phenotype suggests leukotriene contribution. Diphenhydramine is positioned as a defined rescue step for acute symptom spikes.
- In these layered approaches, compounded ketotifen may serve as the stabilization anchor because no commercial oral alternative exists.
Gastroenterologist
- Abdominal pain with post-meal flares and a hypersensitivity-type quality.
- Ketotifen is used as a stabilization strategy for mast-cell involvement, with response evaluated over time rather than by immediate symptom swings.
- When the GI pattern becomes persistent and inflammatory-leaning, budesonide is the targeted escalation step. Rescue planning stays separate and minimal, used only when an acute histamine-type episode is clearly present.
- Gradual titration and excipient control may influence whether stabilization therapy is tolerated long enough to evaluate efficacy.
Internist
- Multisystem flares with urticaria alongside GI symptoms, medication sensitivity, and a persistent symptom burden.
- The plan aims to lower total symptom load without blurring medication roles: ketotifen as baseline stabilization, gabapentin for burden reduction, and diphenhydramine as a clearly defined rescue option for acute spikes.
- Adjunct Strategy: When standard therapies are stable but symptoms remain refractory, LDN (naltrexone) is introduced as a structured, monitored adjunct add-on. Steroid escalation is separated and only reserved for severe situations rather than blended into routine care.
- In multisystem presentations, compounding allows separation of medication roles while minimizing additive excipient burden.
Why a Compounding Pharmacy May Be Central in MCAS Care
Many medications used in Mast Cell Activation Syndrome management fall into one of three categories:
- Not commercially available in appropriate oral form (e.g., ketotifen)
- Available only in fixed strengths that limit gradual titration
- Contain excipients that may trigger symptoms in sensitive patients
Because of these limitations, compounding pharmacies may becomes integral to executing a layered MCAS therapy plan.
In mast cell disorders, success is often determined not only by selecting the correct medication class — but by ensuring the formulation itself does not provoke activation.
Healing Dose Compounding Pharmacy: Michigan’s Reliable Source for Personalized Medications
At Healing Dose Compounding Pharmacy, we provide more than compounded prescriptions. We support prescribers with formulation options to help improve tolerability, adherence, and individualized care for patients with complex allergy, pain, and mast-cell-adjacent symptom patterns.
Why Choose HDRx for Compounded Prescriptions:
- Accredited Pharmacy that supports high standards of quality and safety across compounded formulations.
- Serving multiple states from MI to OH, IN, WI, MN, and FL (Florida: non-injectable dosage forms only).
- Customizing dosing, strengths, and delivery forms to match patient-specific needs under prescriber guidance.

- Offering education to practitioners as well as patients for evidence based decision making.
- Collaborating with allergists/immunologists, family medicine clinicians, and other specialists to support well-structured care plans.
MCAS Care Plans May Require Compounded Formulations
If you’re a patient struggling with hives, itching, and recurring flare patterns, ask your healthcare provider whether compounded formulations may be appropriate for your care plan.
If you’re a prescriber, Healing Dose Compounding Pharmacy is here to support individualized prescribing and formulation strategies for your patients.
In many MCAS cases, the ability to customize strength, remove reactive excipients, and create non-commercial formulations is what makes structured care possible. Contact Healing Dose Compounding Pharmacy today to learn more about compounded medications and prescriber support.
References
- Abella, B. S., Berger, W. E., Blaiss, M. S., Stiell, I. G., Herres, J. P., Moellman, J. J., Suner, S., Kessler, A., Klausner, H. A., Caterino, J. M., & Du, J. (2020). Intravenous cetirizine versus intravenous diphenhydramine for the treatment of acute urticaria: a Phase III randomized controlled noninferiority trial. Annals of Emergency Medicine, 76(4), 489–500. Link
- Badloe, F. M., Grosber, M., Ring, J., Kortekaas Krohn, I., & Gutermuth, J. (2024). Treatment of acute urticaria: A systematic review. Journal of the European Academy of Dermatology and Venereology, 38(11), 2082–2092. Link
- Breneman, D. L. (1996). Cetirizine versus hydroxyzine and placebo in chronic idiopathic urticaria. Annals of Pharmacotherapy, 30(10), 1075–1079. Link
- de Brito, T. V., Júnior, G. J. D., da Cruz Júnior, J. S., Silva, R. O., da Silva Monteiro, C. E., Franco, A. X., … & dos Reis Barbosa, A. L. (2020). Gabapentin attenuates intestinal inflammation: role of PPAR-gamma receptor. European Journal of Pharmacology, 873, 172974. Link
- Erbagci, Z. (2002). The leukotriene receptor antagonist montelukast in the treatment of chronic idiopathic urticaria: A single-blind, placebo-controlled, crossover clinical study. Journal of Allergy and Clinical Immunology, 110(3), 484–488. Link
- Frieri, M., Patel, R., & Celestin, J. (2013). Mast cell activation syndrome: a review. Current allergy and asthma reports, 13(1), 27–32. Link
- Gunal, A. I., Ozalp, G., Yoldas, T. K., Gunal, S. Y., Kirciman, E., & Celiker, H. (2004). Gabapentin therapy for pruritus in haemodialysis patients: a randomized, placebo-controlled, double-blind trial. Nephrology Dialysis Transplantation, 19(12), 3137–3139. Link
- Klooker, T. K., Braak, B., Koopman, K. E., Welting, O., Wouters, M. M., Van Der Heide, S., Schemann, M., Bischoff, S. C., Van Den Wijngaard, R. M., & Boeckxstaens, G. E. (2010b). The mast cell stabiliser ketotifen decreases visceral hypersensitivity and improves intestinal symptoms in patients with irritable bowel syndrome. Gut, 59(9), 1213–1221. Link
- Kuruvilla, M. E., Mathew, S., & Avadhani, V. (2018). Treatment of Refractory Mastocytic Enterocolitis with Budesonide. Journal of Gastrointestinal and Liver Diseases, 27(3), 327–329. Link
- Sadeghian, M., Farahmand, F., Fallahi, G. H., & Abbasi, A. (2008). Cyproheptadine for the treatment of functional abdominal pain in childhood: a double-blinded randomized placebo-controlled trial. Minerva pediatrica, 60(6), 1367–1374. Link
- Tsilioni, I., & Theoharides, T. (2024). Luteolin is more potent than cromolyn in their ability to inhibit mediator release from cultured human mast cells. International Archives of Allergy and Immunology, 185(8), 803–809. Link
- Valent, P. (2013). Mast cell activation syndromes: definition and classification. Allergy, 68(4), 417–424. Link
- Watson, N. T., Weiss, E. L., & Harter, P. M. (2000). Famotidine in the treatment of acute urticaria. Clinical and experimental dermatology, 25(3), 186–189. Link
- Weinstock, L. B., Brook, J. B., Myers, T. L., & Goodman, B. (2018). Successful treatment of postural orthostatic tachycardia and mast cell activation syndromes using naltrexone, immunoglobulin and antibiotic treatment. BMJ Case Reports, 2018, bcr-2017. Link
- Yamada, S., Shirai, M., Inaba, Y., & Takara, T. (2022). Effects of repeated oral intake of a quercetin-containing supplement on allergic reaction: a randomized, placebo-controlled, double-blind parallel-group study. European Review for Medical & Pharmacological Sciences, 26(12). Link
